

Monitoring the patient during anaesthesia is most commonly carried out by a trained veterinary technician or assistant; there must be good communication between the surgeon and the technician as regards to the patient's status under anaesthesia to ensure their safety. As we have discussed in the previous sections, the drugs used can have profound effects on physiological parameters. Monitoring will enable the detection of early signs of an impending issue and enable the appropriate action to be taken to avoid it, thereby reducing the incidence of morbidity and mortality.
Patients that are sedated or anaesthetised must be monitored continuously and physiological parameters recorded on the anaesthetic record sheet every 5 minutes. Never be complacent!
The patient is monitored by assessing a range of physiological parameters. Whilst clinical reference values are used as a guide to what is a 'safe' range for these parameters whilst under anaesthesia, be aware that each patient is different, and that looking for changes in trends will enable the anaesthetist to pre-empt a problem and deal with it before it becomes more serious.
The aims for monitoring anaesthesia are to:
- Depth. Maintain appropriate anaesthetic depth for the surgical procedure being performed; this will vary depending on how painful the procedure is. For example, a deeper plane of anaesthesia is necessary during a painful procedure, such as loosening the ovarian ligament or ligation of the testicular vessels and nerves.
- Physiology. Maintain basic physiological parameters within safe limits, which are as close to normal as possible, for example cardiovascular respiratory parameters and core body temperature.
- Perfusion. Ensure continuous and adequate perfusion of tissues to support the metabolism of vital and non-vital organs.
- Patient safety. Protect the safety of the patient.
- Staff safety. Protect the safety of staff by ensuring that the patient is fully unconscious and cannot respond to surgical stimuli.
Basic monitoring requires very little equipment; the focus is on the assessment of clinical parameters - reflexes, body temperature, pulse and respiration values. It is always better to monitor these parameters rather than to rely on equipment solely to assess the patient.

Normal parameters
The table below outlines the range of parameters considered normal for dogs. Remember that changes in trends rather than absolute values are key to predicting and preventing an issue before it occurs.
Monitoring the respiratory system
The lungs are critical for absorbing oxygen for delivery by the bloodstream to vital organs, and for carbon dioxide to be removed as a waste product. This gaseous exchange is called ventilation.
The respiratory system can be assessed by observing:
Breathing rate
The breathing rate can be assessed by a number of methods: visual assessment of movement of the chest wall; placement of a piece of tissue paper in front of the nose to watch for movement during expiration; or if the patient is being maintained on gaseous anaesthesia, the movement of the rebreathing bag can be monitored.
Particular attention needs to be paid to any brachycephalic dogs. Anatomical abnormalities in the upper airways (elongated soft palate, stenotic nares, hypoplasia of the trachea, excessive laryngeal folds) may cause obstruction of the airways under sedation and anaesthesia. These patients should always be intubated immediately after induction and extubated only after the swallowing reflex has returned.
If the breathing rate starts to increase (tachypnoea), this can be due to:
- depth of anaesthesia is insufficient
- a response to a painful procedure
- Hypercapnia (excessive carbon dioxide in the blood)
If the breathing rate starts to decrease (bradypnoea), this can be due to:
- depth of anaesthesia is too great
If the breathing rate stops (apnoea), this can be due to:
- depth of anaesthesia is too great
- certain drugs, such as opioids or Propofol
- impending cardiac arrest
- depth of anaesthesia is insufficient and the patient is breath holding
What about respiratory effort? Assess the degree of effort the patient is having to make in order to breathe. If it is having difficulty in breathing (dyspnoea), the abdomen will move excessively in order to try and improve oxygen intake. This is an emergency and immediate action must be taken. Causes can include:
Mucous membrane colour
Colour of mucus membranes (gums and conjunctiva) provides some information about peripheral perfusion:
Pale pink – white: Haemorrhage, hypoperfusion, anaemia, inadequate analgesia

Brick red: Sepsis, hypercapnia (increased carbon dioxide in the blood)

Blue: Hypoxaemia (inadequate oxygenation of the blood); also referred to as cyanosis

Monitoring the cardiovascular system
Heart Rate
Every patient should have their heart and pulse rate taken and the heart auscultated before medications are given; however, as discussed previously, this may not be possible with all animals in an ABC setting due to their temperament. Therefore, under these circumstances, these parameters should be assessed immediately after the animal is fully sedated.
Every anaesthetist should have a stethoscope ready and use it. The heart rate can be monitored by auscultation using a conventional stethoscope (Figure 5), an oesophageal stethoscope, or by palpation of the heart at the apex beat on the left thoracic wall.

Using an oesophageal stethoscope
This is a device for monitoring the heart rate, rhythm and character. It comprises a flexible, thin tube; at one end, the tube contains small holes covered by thin plastic, (Figure 6). The other end connects to stethoscope earpieces by using a small adaptor. It is cheap and easy to use and come in various sizes. The advantage of an oesophageal stethoscope is to be able to directly auscultate the heart without disturbing surgical drapes.

- Ensure that the tube is fed into the oesophagus and not the trachea.
- Place the stethoscope after ET intubation has been completed.
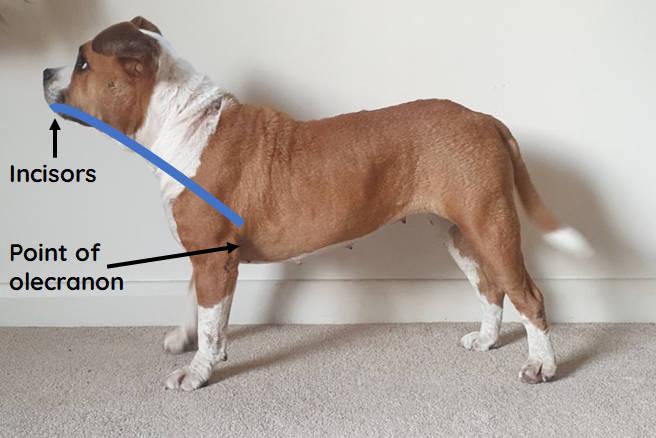
- Do not insert it too far down as this can result in placement in the stomach which disrupts the function of the cardiac sphincter and can result in gastric reflux and oesophagitis. As a guide, measure from the incisors to the point of the olecranon (Figure 7).
Assessment of pulses
Palpation of a central pulse such as the femoral pulse, at the same time as assessing the heartrate, is useful for assessing their synchronicity (Figure 8).

- A high heart rate (tachycardia) can indicate an inadequate depth of anaesthesia i.e. the patient is too light, inadequate analgesia, hypotension (shock, sepsis), hypercapnia or hypoxaemia. It can also increase in response to certain drugs e.g. ketamine.
- A lower than expected heart rate (bradycardia) can be caused by too deep a plane of anaesthesia, hypothermia, hypertension (reflex bradycardia), hyperkalaemia, side effects of certain drugs e.g. alpha-2 agonists, vagal stimulation (pressure/stimulation of the vagal nerve during surgery or the eye, neck or gastro intestinal tract, this should resolve once the pressure is released).
Peripheral pulses provides information about the peripheral circulation and cardiac output. The following arteries are commonly assessed:
- Metacarpal artery: located lateral to the dew claw on the palmar aspect of the forelimb (Figure 9).
- Dorsal pedal artery: medial aspect of the metatarsus (Figure 10).
- Labial artery: found on the inside lip just caudal to the level of the upper canine tooth.
- Lingual artery: midline on the ventral aspect of the tongue.
- Coccygeal artery: ventral aspect of the tail base.


As peripheral pulses are more sensitive to change than central pulses, it is possible to detect and avoid an impending crisis if any change in peripheral pulse quality is perceived. This is because peripheral pulses will be modified by low blood pressure or poor perfusion as compared to a central pulse, such as the femoral artery. However, when peripheral pulses can not be assessed, central pulses are still useful.
Capillary Refill Time (CRT)
To perform this assessment, fingertip pressure is applied to blanch the gum of the patient; when the finger is removed, the time taken for the area to return to its previous pink colour should be less than 2 seconds in a healthy patient. Prolonged refill time is suggestive of:
- cardiovascular issues
- hypovolaemia
- poor peripheral perfusion
- shock
- hypothermia.
Assessment of reflexes
Jaw tone
Carefully open the jaws of the animal (Figure 11). If there is resistance, the patient is in a light plane of anaesthesia. The jaw tone reduces with an increased depth of anaesthesia. Importantly, animals anesthetised with ketamine protocols will still have jaw tone, even at adequate depths of anaesthesia (see our Quick Reference download on monitoring patients anaesthetised with ketamine).

Palpebral reflex
Gently tap the medial canthus of the eye (the corner of the eyelids near the nose). If the blink is strong, then the patient is in a light plane of anaesthesia. If it is absent, the patient is deeply anaesthetised. Again animals anaesthetised with ketamine will retain a palpebral reflex even at adequate levels of anaesthesia (see out Quick Reference download on monitoring patients anaesthetised with ketamine).
Pedal reflex
Gently extend the limb and pinch the webbed skin between the toes to inflict pain. If the leg moves away from the stimulus, the patient is in a light plane of anaesthesia.
Eye position
Open the eyelids and assess how the eye is positioned. If the eye is rotated down, in a ventromedial position this is usually consistent with an appropriate level of surgical anaesthesia. When the anaesthesia increases in depth, the eyes will become central again.
If the eyelids are open and the eyes are “staring” straight ahead, the level of anaesthesia may be very light or too deep - immediately test the palpebral reflex. If it is strong, the patient is light; if there is no palpebral reflex, the patient is too deeply anaesthetised and at risk of cardiorespiratory arrest. In this instance, check other reflexes and take appropriate action rapidly.
Remember that ketamine interferes with this relationship and the eye will usually remain central regardless of depth of anaesthesia.
Monitoring body temperature
Rectal temperature should be taken during of the anaesthetic period, and measurements to prevent/correct an abnormal temperature should immediately be taken. A simple rectal thermometer is all that is needed.
Body temperature is one of the easiest parameters to monitor, yet is often overlooked!
Measures to prevent heat loss should be taken from the time of premedication. Hypothermia (anything below 37°C in dogs and cats) during general anaesthesia is not uncommon but is easy to prevent in routine cases. This can be achieved using using warming aids such as bubble wrap around the feet, legs and head, insulating the table, or by covering the body with blankets during recovery (blankets should not be used in an aseptic theatre). Some commercial methods are available that use active warming systems 'HotDog Warming system', but these are unlikely to be available in a spay-neuter setting.
It is thought that heat loss occurs most quickly in the first 30 minutes of anaesthesia; therefore, even patients that are having a quick, routine procedures, their body temperature continues to decrease during recovery.
Particular attention must be paid to compromised, young, geriatric and small animals, all of whom are at increased risk of hypothermia.
There are many deleterious effects of hypothermia, including those that involve the cardiovascular, neurological and immune body systems which can lead to a prolonged recovery and an increase in the risk of post-operative complications. We can avoid these using simple methods:
Warm up IV fluid bottles by immersing them in hot water before inducing the patient (Figure 12). They should feel very warm to the touch. Bottles should be sealed or kept upright so that the fluids are not contaminated by the hot water. During a long surgery the fluids may need to be reheated or the hot water bottle may need to be changed.
Place a hot water bottle directly on the IV fluid line as close as possible to the IV catheter.
Take care that the hot water bottle does not come into direct contact with the patient as this can cause severe burns.

Use warming aids such as bubble wrap or newspaper around the feet, legs and head (Figure 13).

Position the animal on an insulating surface such as newspaper or clean blanket, and not directly onto the operating table.
Additional automated equipment
Pulse oximeter
Pulse oximeters may be available to use in a spay-neuter setting and is commonly used in veterinary practices. They provide a non-invasive method of measuring the oxygen saturation of haemoglobin (referred to as SpO2). It evaluates the amount of oxygen that the blood is carrying compared to the maximum level, and displays this as a percentage of the maximum. Oxygen saturation value assessment can detect hypoxia, which is a common endpoint for many pathophysiological disturbances during anaesthesia. It is therefore a useful monitoring tool.
The oximeter emits infrared and red light at different wavelengths. The haemoglobin absorbs different wavelengths depending on whether it is attached to oxygen; a photodetector detects the remaining wavelengths and converts this into a percentage output.
The probe must be placed on a non-pigmented area; a commonly used site is the tongue (Figure 14); the vulva, prepuce, interdigital skin and ear pinnae can also be used (don't forget to clean the probe between patients).

The aim is to maintains SpO2 above 95% saturation. If the reading falls below this level, check the following:
- Are there clinical signs to support a low oxygen saturation i.e. cyanosis? If yes, act immediately.
- If not, reposition the probe. Often, they can display anomalous results and re-positioning will result in an improved reading.
Always use the basic monitoring parameters (respiratory and cardiovascular system) in addition to automated readings from a pulse oximeter to help interpretation.
Many pulse oximeters show a plethysmograph waveform, and assessment of the shape of the waveform is more important than looking at the number. A good pulse waveform is demonstrated in Figure 15, where the corresponding number of 99% is likely to be accurate. If the number is high but the waveform is poor, measures should be taken to try and confirm accuracy, such as clinical signs and repositioning the probe.

Downloadable resources for anaesthetic monitoring
Download and use our free resource guides on general anaesthetic monitoring and monitoring of animals anaesthetised with ketamine.