

What is ORS?
Ovarian remnant syndrome (ORS) describes a collection of clinical signs resulting from the retention of functional ovarian tissue inside a bitch after performing an incomplete ovariohysterectomy (OHE) surgery.
There are a number of suggested reasons why this occurs:
- By far the most common cause is failure to remove all of the ovarian tissue during surgery. As the right ovary and uterine horn are located more cranially than their left counterparts, this ovary, in particular, is predisposed to being incompletely removed.
- Failure to remove ectopic, extraovarian tissue during surgery. Ectopic tissue is tissue that is located in an abnormal location and therefore may not be noticed when the surgeon removes the ovaries.
- Revascularisation of the ovarian tissue that is left in the abdominal cavity.
When dogs retain ovarian tissue, they continue to display intermittent clinical signs associated with their oestrus cycle, such as swelling of the vulva and serosanguineous vaginal discharge. They will also show normal behaviour patterns, such as flagging, standing, and attracting male dogs.
The remnant ovary can result in a range of pathologies, such as promoting the development of a granulosa cell tumour, mammary neoplasia, and stump pyometra. If an ovariectomy and not a full OHE has been performed, the uterus remains in situ and the bitch has the potential to become pregnant.
Diagnosis
Diagnosis is based on a number of factors which include a full history, clinical signs, vaginal cytology, abdominal ultrasound, hormonal analysis, and exploratory laparotomy. Not all of these options may be available to you, but they will be discussed in more detail below, including their limitations in their usefulness of diagnosing ORS, to help guide you.
1. Physical examination
A physical examination of a bitch ‘on heat’ will include vulvar swelling and serosanguinous vaginal discharge. They will otherwise be bright and healthy. However, during anoestrus, these signs will be absent in a patient with ORS, so absence of clinical signs does not rule it out.
2. Vaginal cytology
As with the physical exam, vaginal exfoliative cytology can be performed to aid in diagnosing ORS. The epithelial layer of the vagina is affected by changes in the blood concentration of oestrogen as it prepares the vagina for mating. By studying the appearance of these cells from a vaginal smear, we can confirm whether oestrogen is present.
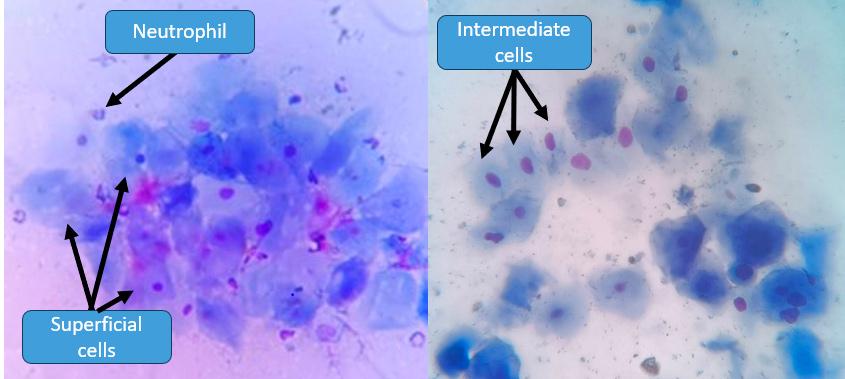
When blood oestrogen levels are increasing, such as proestrus followed by oestrus, there is a shift of cells from parabasal (small cells with large nuclei) and intermediate cells (larger cells with a ‘fried egg’ appearance) to keratinised, epithelial cells, known as superficial cells (Figure 1). Superficial cells have a cornified appearance with their nuclei becoming pyknotic/absent. In addition, red blood cells and neutrophils are often observed, particularly in proestrus.
3. Abdominal ultrasound
Abdominal ultrasonography is useful in assessing for the presence of remnant ovarian tissue. However, in resource limited settings, this option may not be available. The effectiveness of the procedure depends on the expertise of the examiner, the size of the remnant tissue, and the stage of the oestrus cycle. For example, the presence of a suture granuloma at the ligation site can lead to a false positive identification of remnant ovarian tissue.
An example of the appearance of an ovarian remnant is shown in Figure 2, which appears as a hypoechoic, cystic structure on the caudal pole of the right kidney.

4. Sex hormone serology
Demonstrating the presence of key hormones in the blood can also be used as a diagnostic tool. There are a number of hormones that can be assayed; however, they are all limited in their usefulness:
Anti-Müllerian Hormone (AMH). Complete removal of ovaries should result in the absence of AMH in the circulation. A positive result from a single serum sample to measure AMH can help diagnose dogs and cats with ORS. However, AMH expression is limited to granulosa cells of ovarian follicle, and not in the corpus lutea. Therefore, an ovarian remnant that is largely occupied by luteal tissue might not secrete a sufficient amount of AMH to be detected in the circulation. Therefore a negative result should be treated with caution.
Luteinising Hormone (LH). LH assay will be positive for only a short period during the transient, pre-ovulatory LH peak in intact bitches and those with ORS, and will be absent in spayed animals.
Progesterone (P4). Progesterone is produced by the post-ovulatory corpus luteum. Confirmation of ovarian tissue by serum P4 requires the bitch to either be in dioestrus or pregnant. There won’t be a significant difference in serum P4 levels between spayed and intact, anoestrus queens and bitches.
5. Responsive serology testing
Responsive serology testing can be performed by administering an injection of gonadotropin hormone-releasing hormone (GnRH), and then measuring the serum samples of P4 or luteinising hormone (LH) levels. This is often a costly option.
It has been found that measuring the combination of serum AMH and progesterone is superior to measuring either hormone individually (Place, 2019). In a study of 602 dogs, 48 dogs were confirmed to have ORS using histopathology. Of these, 52% were positive for both hormones, 35% were positive for at least one of the hormones, and the rest had at least one inconclusive result. None of the dogs with ORS were negative for both hormones.
Treatment
Exploratory laparotomy
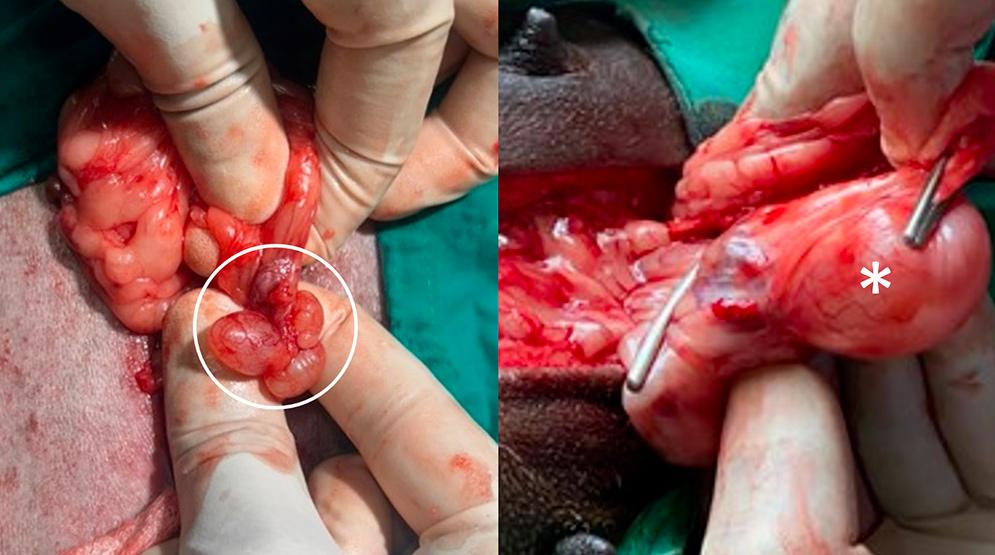
Exploratory laparotomy is a method for both confirming the presence of ORS, and resolving the condition through complete surgical removal of the remnant, ovarian tissue.
The recommended time for exploratory laparotomy is post-ovulation, around 2 to 4 weeks after the bitch comes out of heat, as this is when the remnant is easily located.
Under general anaesthesia, the patient is placed in dorsal recumbency and the surgical site is clipped and scrubbed with chlorhexidine followed by isopropyl alcohol spray. A ventral midline celiotomy incision is performed with the incision site located in a more cranial position than that chosen during a routine OHE; this is to ensure the surgeon can more easily locate the ovarian remnant which normally located on the caudal pole of the kidney, in particular the right kidney. Note that great care must be taken to identify the ureter prior to resecting the ovarian remnant to avoid inadvertent ureteral damage.
Remove the ovarian remnant, ensuring no further tissue remains in situ. The pedicle ligation is performed using 2-0 or 3-0 PDS (polydioxanone). The muscle and subcutaneous tissue are closed in simple continuous pattern and the skin is closed with intradermal pattern using PDS 1-0 . A course of post operative analgesics is prescribed for the animals undergoing ORS surgery.
An alternative, laparoscopic approach has shown to be effective in successful identification and removal of ORS by a suitably experienced surgeon. This has the added advantages of a short convalescence period and a reduction in the risk of complications compared to the conventional, invasive, open surgical procedure. However, in a high throughput, spay/neuter facility, this may not be an option due to lack of equipment and expertise.
Histopathology
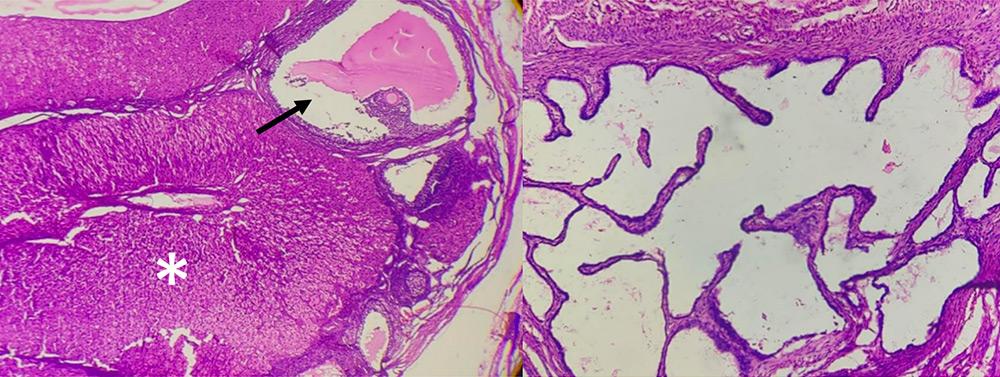
The resected ovarian tissue should immediately be placed in 10% neutral-buffered formalin (in a minimum of 1 volume of tissue to 10 volumes of formalin) and sent for histopathological examination. Analysis of tissue sections on slides stained with haematoxylin and eosin can confirm the presence of ovarian tissue, as shown in Figure 4.
Prognosis
The prognosis is excellent if the remnant ovarian tissue is completely removed. There is no published data about the reoccurrence of ORS in companion animals.
Prevention
Although this is described as a ‘syndrome’, ORS is an iatrogenic condition that can be prevented through proper surgical techniques. All surgeons should use good techniques, such as sufficient surgical incision and proper clamp placement, and always seek the assistance of a more senior colleague if they are unsure. In this way, ORS can be avoided.