

Canine Distemper Virus (CDV) is a highly contagious viral pathogen that is able to cross species barriers and have a widespread impact on both domestic and wildlife animal populations. Due to the large number of susceptible species, these species can become a reservoir for infection and perpetuate its presence.
Pathogenesis
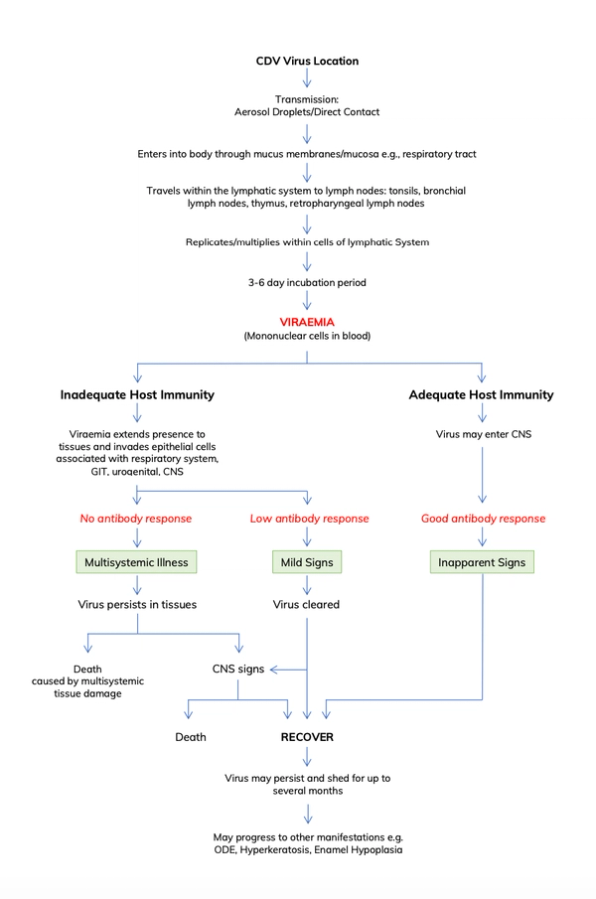
CDV is a fragile, single-strand RNA virus, and is thus relatively unstable outside the host. It can be destroyed by lipid solvents, most disinfectants, and through desiccation from sunlight exposure; it can last up to seven hours in the environment. It therefore prefers cooler and more moist environments/seasons where it can persist for longer. Infected dogs can shed the virus for several months. The virus can be spread by three particular methods:
- Aerosol droplet secretions from infected animals; through coughing or sneezing
- Direct contact with infected animals
- Through the placenta
The virus initially replicates in the lymphatic system of the respiratory tract where it often gains entry. After a 3-6 day incubation period, a viremia then extends its presence and impact to the gastrointestinal, urogenital, and neurological systems. Disease will follow once the virus replicates within these tissues.
Clinical Presentation
The clinical symptoms are dependent on the viraemic stage of the disease and what tissues it replicates within. The symptoms can be split into different body systems in a chronological order as follows. Note that these are seen in the acute infection:
Pyrexia (a diphasic fever) – a transient fever occurs 3-6 days after infection and is often missed. There may also be a lymphopenia at this time and is accompanied by an anorexia; it subsides within a few days. A second fever occurs after several days and is then often accompanied by more systemic signs.
Respiratory Symptoms
- Mucopurulent ocular discharge
- Serous nasal discharge
- Coughing
- Sneezing
Gastrointestinal Symptoms
- Vomiting
- Diarrhoea
Neurological Symptoms (encephalomyelitis)
- Nystagmus
- Involuntary muscle spasms – e.g. masseter/temporalis muscle spasms with marked jaw tone
- Paresis or Paralysis
- Seizures – ‘lip-smacking’ or ‘chewing-gum’ fits
A longer course of illness is associated with the presence of neurological signs, but there is no definitive way to determine if CDV will manifest itself with neurological symptoms within a certain dog.
Other manifestations:
- ‘Hard Pad disease’ – if the dog survives and recovers from the acute phase of the disease, they can then develop hyperkeratosis of the pads and nose, enlarging the pads that can cause discomfort.
- Enamel Hypoplasia – this is often seen in puppies who have fortunately survived the virus. The fever associated with CDV at the time that their enamel is developing leads to poor enamel growth at that period. This is often seen as a ring around the tooth and affects several teeth.
- Old Dog Encephalitis (ODE) – a chronic form of CDV that often presents with ataxia, compulsive circling or pacing, and head-pressing. This is a disease that can be seen in older dogs without a history of CDV, but who have recovered from an infection when exposed at a younger age. The disease presents much later in life as a result of an immune-mediated inflammatory response to a persistent CDV presence in the CNS. The virus itself is relatively dormant and not replicating, thus the dogs is not infectious nor shedding the virus. The exact mechanisms behind the trigger of this syndrome are not currently known.
Diagnosis
The diagnosis of CDV is typically through identifying its clinical manifestations. It should always be considered in a febrile dog presenting with multisystemic disease, particularly in high risk areas with an unvaccinated population.
Other options include:
- Antigen Rapid Test - quick, straightforward, and applicable for field environments
- RT-PCR - the most definitive diagnostic test for CDV although it is not often available.

Treatment
Treatment for CDV is almost conclusively symptomatic and supportive. Unfortunately, treatment once the symptoms have become neurological is often unsuccessful, and if these symptoms are progressive or severe, welfare needs to be taken into consideration with the owner.
Nonetheless, with prompt and aggressive care, some dogs may recover from multisystemic manifestations, with or without long-term neurological tremors. Treatment will include:
- IVFT with appropriate electrolyte solutions
- Hartmanns Solution/Lactated Ringers: 2-5ml/kg/hr
- Broad-Spectrum Antibiotics
- Amoxicillin-Clavulanic acid: 20mg/kg PO/IV/SC every 8-12 hours
- Doxycycline: 5-10mg/kg PO/IV every 12 hours
- Analgesics
- Buprenorphine: 0.02mg/kg IV every 6-8 hours
- Methadone: 0.1-0.3mg/kg IV every 4-6 hours
- Paracetamol: 10-20mg/kg IV every 8 hours. Paracetamol should not be the first choice for analgesia, but is here for cases where pain and discomfort is not being managed successfully and multimodal analgesia is required
- Anticonvulsants
- Diazepam: 0.5-1mg/kg IV administered as a bolus and repeatable up to 3 times within no less than 10 minutes. This is for immediate management of convulsions and will sedate
- Midazolam: 0.2-1mg/kg IV. This is for immediate management of convulsions and will sedate
- Phenobarbitone: 2mg PO/IV every 12 hours. Note that phenobarbitone is useful for longer-management of convulsions, and diazepam may have to be used in conjunction for more immediate management
- Antipyretics – paracetamol (cautious of using NSAIDs if GI signs are severe)
- Paracetamol (as above): 10-20mg/kg IV every 8 hours. Paracetamol is an adjunct for multimodal analgesia, but also useful as an anti-pyretic in pyrexic animals
- Steroids (CAUTION) Lower doses are more anti-inflammatory (0.5-1mg/kg) - Higher doses are more immunosuppressive (1-2mg/kg).
- Dexamethasone: 1-2mg/kg IV every 24 hours. This is often used in critical cases of CNS oedema or associated inflammatory meningitis, both in active infections and also in ODE where it is the immune response causing disease rather than the virus. Prior to use, the patient condition must be thoroughly clinically analysed on whether it is truly essential due to its immunosuppressive potential
- Prednisolone: 1-2mg/kg PO every 12-24 hours. Identical risks stated above
Prognosis
The prognosis does depend on certain variables such as age, immunocompetence, and clinical presenting signs. Nonetheless, the prognosis is always very poor, and worsens if the animal presents at the stage of the disease where neurological manifestations are present.
Prevention
Vaccination is the key to prevention. Widespread vaccination is important in populations, not only to prevent disease, but to also prevent reservoirs existing within a domestic population. See our vaccine page for more information.