

Key Points
- Haemostasis initially involves intense vasoconstriction, to stop bleeding.
- After this, an increase in vascular permeability and vasodilation during the inflammatory stage allows immune cells to quickly migrate to the wound. The inflammatory stage prepares the wound for healing, and lasts for around 5 days (though it may vary).
- It is normal for wounds in this stage to appear red, swollen, hot and they may be painful.
- Neutrophils, macrophages and lymphocytes work to remove micro-organisms, and tissue debris from the wound, and modify the tissue to become a healthy bed for granulation.
Haemostasis
In the first few minutes after injury, the body stops bleeding (haemostasis) through the following steps:
- Reflex vasoconstriction occurs within the first 5-10 minutes. Capillaries around the wound narrow to reduce blood flow, limiting blood loss.
- Signals released by damaged endothelial cells (on the inner surface of capillaries) cause platelets to stick to the injury site. Platelets clump together to form a temporary platelet plug.
- Nearby blood vessels can now expand (vasodilate) to allow oxygen, immune cells and relevant molecules to enter the site of injury and aid healing.
- Further signals released by the damaged endothelial cells trigger a series of reactions known as the coagulation cascade. Fibrin is recruited to the platelet plug, strengthening it. A fibrin plug is formed, as a matrix of activated platelets, red blood cells, fluid, and fibrin.
Functions of the fibrin plug:
- Provides a barrier to infection and further fluid/blood loss.
- Stabilises the wound edges.
- Provides a provisional extracellular matrix, facilitating the migration of immune and tissue cells into the wound.
- Dries to form a protective scab at the surface, which eventually falls off when new, healthy tissue has been formed.

Inflammation
Early Inflammation
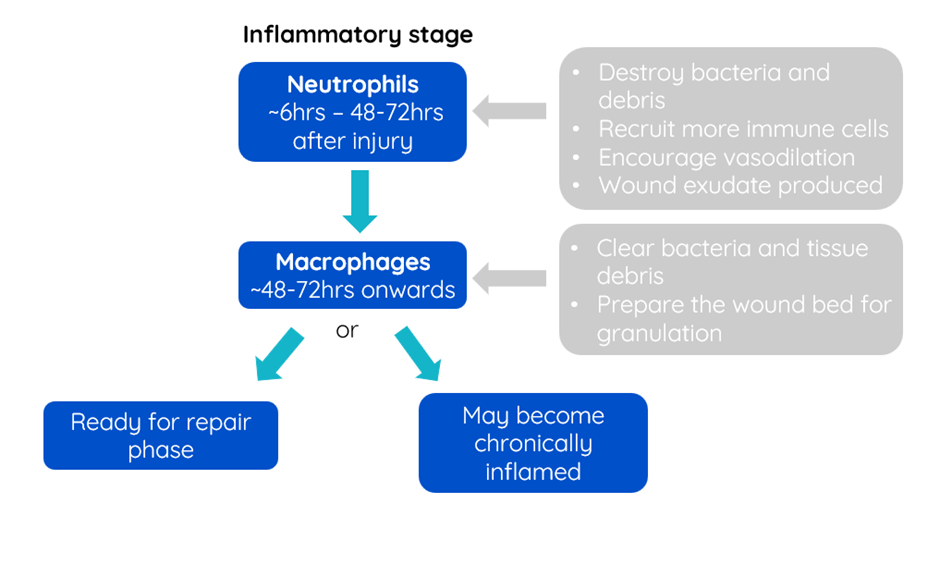
Neutrophils are the first immune cells to arrive at the site of the wound. They arrive in the first six hours after injury, and their concentration peaks about 24-48hrs later. They destroy and phagocytose bacteria, whilst also clearing extracellular debris. In addition, they release pro-inflammatory mediators which encourage vasodilation and the recruitment of more immune cells to the area.
Cytokines: these are small protein molecules which are released by many cells in the body, including immune cells. They are important in cell-signalling. They can act on the cell which secreted them, nearby cells, or cells which are in a distant part of the body. They are important in the process of inflammation, as well as other functions of the immune system.
The degraded neutrophils, dead tissue and wound fluid will create a wound exudate, and this may be purulent (made of pus) primarily due to the presence of neutrophils. A large volume of purulent exudate can be indicative of an infection, although the presence of neutrophils is a normal part of inflammation, even in non-infected wounds. Other factors such as persistent foreign debris can also cause the formation of pus, including abscesses.
Late Inflammation
At around 48-72 hours after the initial insult, neutrophils become less common, and there is an increase in the number of monocytes arriving at the wound. Monocytes transform into macrophages when they reach the site of injury. Lymphocytes may also migrate to the wound to target specific pathogens.
Macrophages continue the process of clearing bacteria and tissue debris (e.g. necrotic material). They will proliferate if foreign debris or bacteria persist. Macrophages also help prepare the wound bed for future granulation by releasing growth factors and cytokines which sustain the inflammatory process and stimulate tissue repair. This starts the process of transforming the initial extra cellular matrix (i.e. the fibrin plug) into granulation tissue, and moving the wound into the next stage of healing (repair).

By the end of the inflammatory stage, if there are no complicating factors to slow down healing, the wound will be ready to begin repair and enter the next stage of healing. However, in cases of infection, persistent foreign material, or large-scale tissue damage, the inflammatory phase may be unsuccessful and therefore become chronic. Wounds sometimes become ‘stuck’ in the inflammatory phase, and require veterinary intervention to encourage the wound to move into the next stage. Advice on how to do this will be covered in the further modules of the course.