

Positioning aids
Positioning aids help to hold patients in place and allow practitioners to move away to avoid scatter radiation. Positioning aids include:
Sandbags. These are used to weigh down patients' limbs, to help keep them in position.
Foam wedges and blocks. These can be placed under a patients' sternum to prevent rotation of the spine. They may also be placed between limbs to raise one or the other.
Rope ties. These can be used to pull limbs forward and tie them so they are out of the collimated field.

Radiographic Views
A radiographic view is the projection the clinician sees when viewing the image. The radiograph can be taken with the patient in a number of positions and angled in different ways to provide different radiographic views for visualising pathology in different anatomical areas. The most commonly used views are:
Dorsoventral (DV). The patient is lying in sternal recumbency, with its sternum on the X-ray plate (belly down). The beam passes straight down through the patient, entering dorsally and exiting ventrally (hence the name which follows the direction of the beam). The patient's front legs are extended and may be secured in place with positioning aids. The left/right marker is placed on either side of the patient to orient the radiograph.

Ventrodorsal (VD). The patient is lying in dorsal recumbency, with its back on the X-ray plate and legs in the air. The beam passes straight down through the patient, entering ventrally and exiting dorsally. The left/right marker is also placed to show the interpreter which side is which.


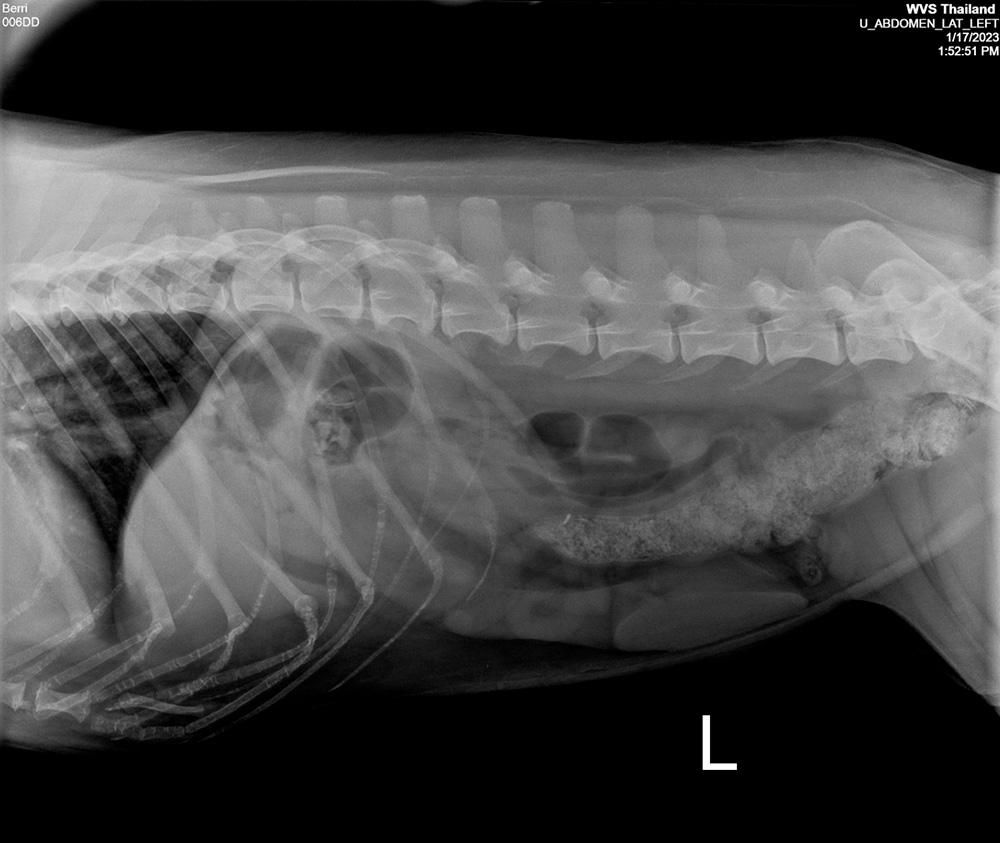
Right lateral. The patient is lying on its side, with its right side touching the X-ray plate. This is the name for both the patient's position and the radiographic view. The right marker is placed in the collimated field.
Left lateral. The patient is lying on its side, with its left side touching the X-ray plate. The left marker is placed in the collimated field.

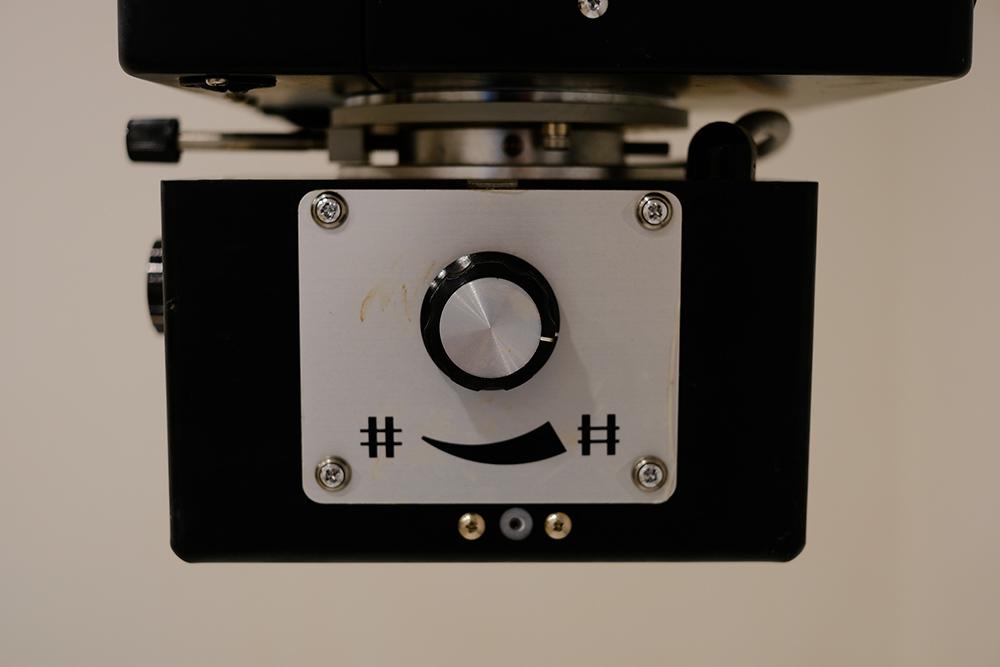
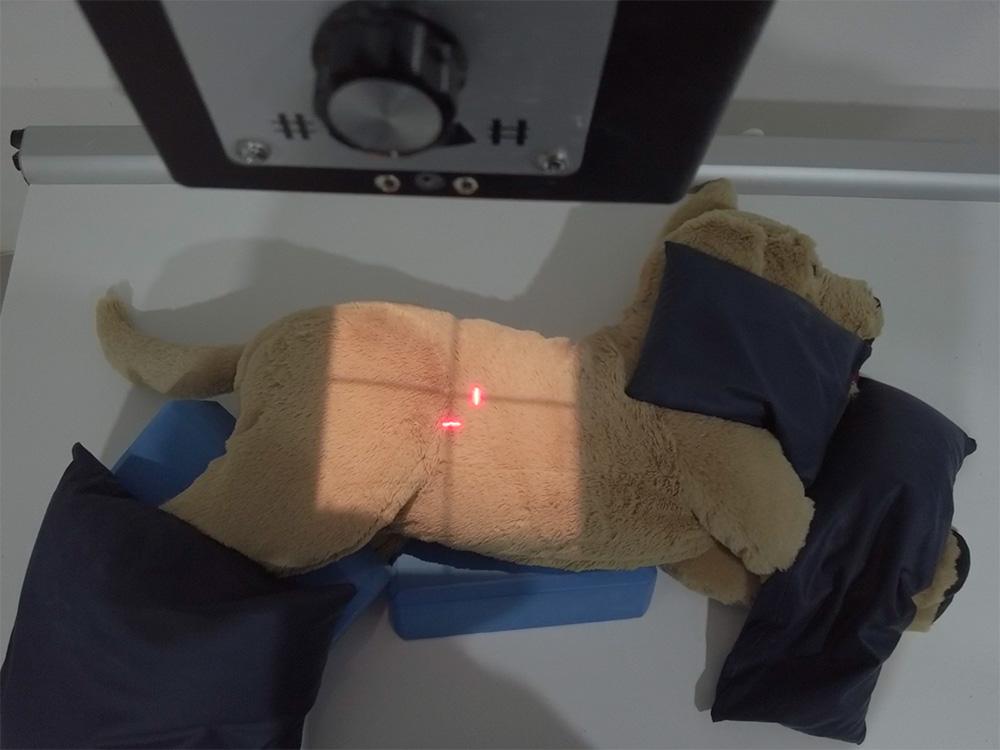
Collimation
Once the appropriate view has been selected, with the patient positioned suitably, the practitioner collimates the primary beam to include the site of interest. This means they adjust the size of the beam and it is done with dials found on the X-ray generator. Light from the generator represents the area that will be exposed. Different radiographs (abdominal, thoracic) require different collimation, and these will be discussed in their respective sections. Clinicians should collimate to only include the site of interest, in order to reduce the radiation dose received by the patient and the associated scatter radiation.
Orthogonal views
We want to gain a 3-dimensional representation of the patient using 2-dimensional images. From a single image, it is not possible to say where a lesion is, due to the overlapping of structures. Therefore, for every patient that is radiographed, we should ensure at least two x-ray images are taken at 90 degrees from one another (orthogonal views). For example, we might take a dorsoventral radiograph along with a right lateral radiograph, which lets us see both the transverse and dorsal planes, and more accurately describe and localise any lesions. Furthermore, some lesions may be missed in certain views and only visible in others, further highlighting the need for orthogonal views to be taken.
Click on the bullets or arrows below to navigate between slides.